 Home >
Solutions - Microwave Ablation - MWA in Lung
Home >
Solutions - Microwave Ablation - MWA in Lung
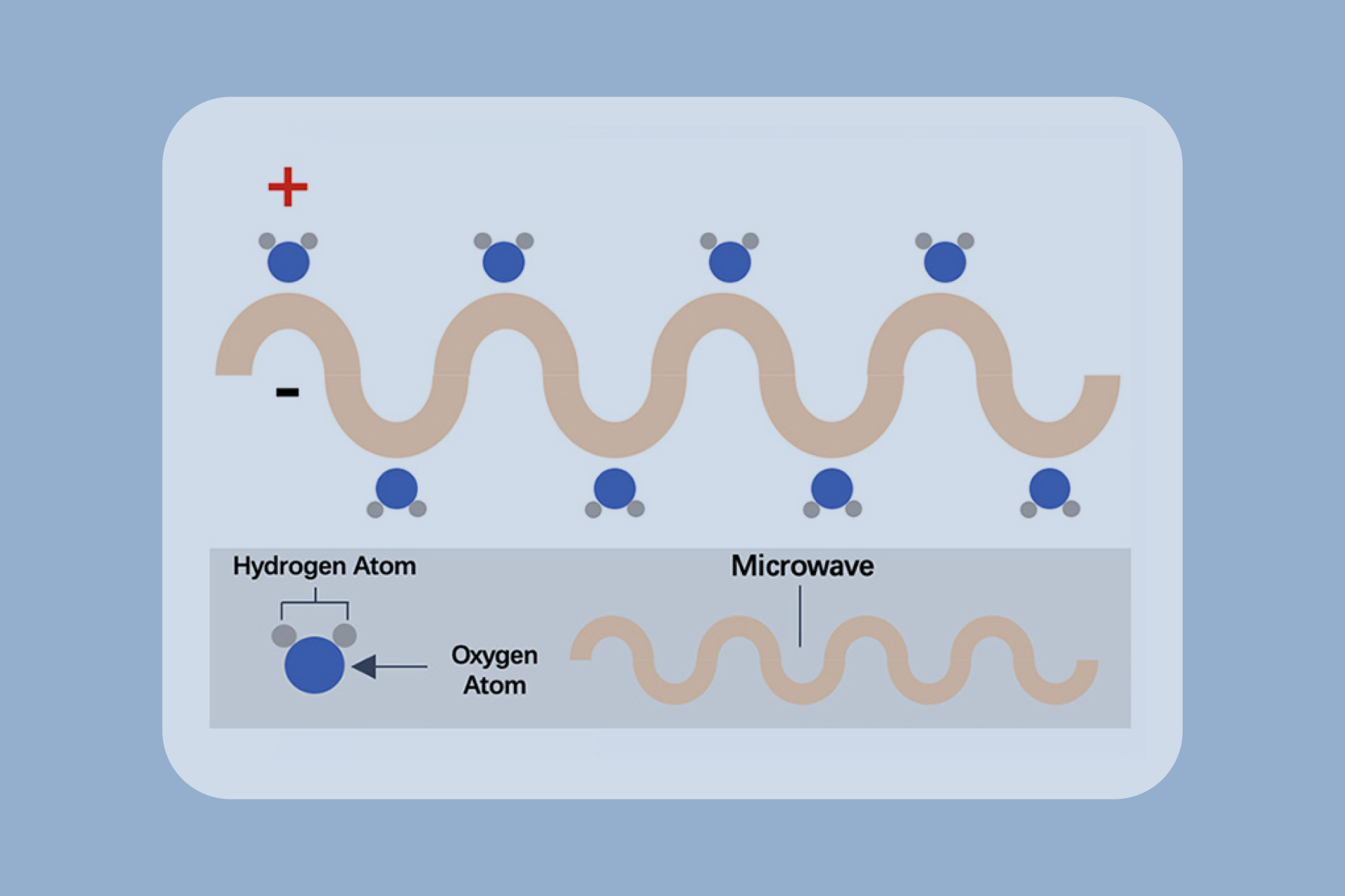
Microwave ablation refers to the use of the electromagnetic methods for inducing tumor destruction by using devices with frequencies of at least 900 MHz to produce tissue-heating effects [5]. Currently, 2450MHz is the frequency used by mainstream products worldwide.

CT of an 80-year-old woman with right upper lobe adenocarcinoma at stage IA (cTlaNOMO). (a) The MWA antenna is shown centrally positioned within the tumor [8]. (b) Ground-glass opacity around the tumor and cavity ni the core was observed ni the image obtained immediately postablation. (c) The axial CT with lung window showed expected thermal damage around the target lesion, without pneumothorax, 24 hours postablation. (d) The enhanced CT image at one month after MWA; the size of the ablation zone was larger than the target tumor but was not enhanced. (e-g) The images at six, 12, and 91 months after MWA; the ablation zone shrank continuously and remained nonenhanced.
Advantages
Reduce morbidity and mortality

Suitability for imaging guidance

Shorter hopitalization stay

Synergy with other cancer treatments

Repeatability
Cost effectively










 Video
Video