MWA in Breast
 Home >
Solutions - Microwave Ablation - MWA in Breast
Home >
Solutions - Microwave Ablation - MWA in Breast
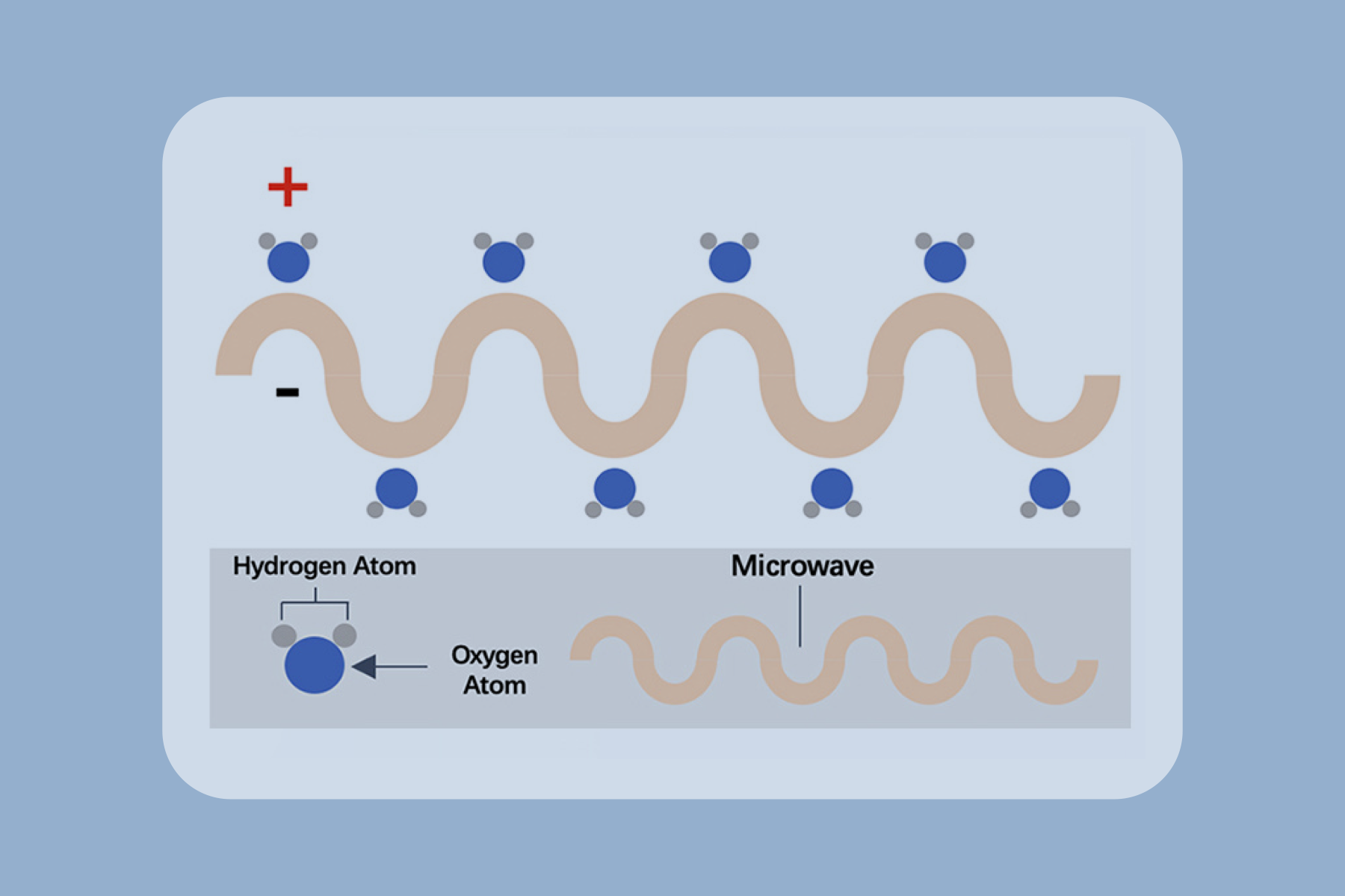
Microwave ablation refers to the use of the electromagnetic methods for inducing tumor destruction by using devices with frequencies of at least 900 MHz to produce tissue-heating effects [4]. Currently, 2450MHz is the frequency used by mainstream products worldwide.
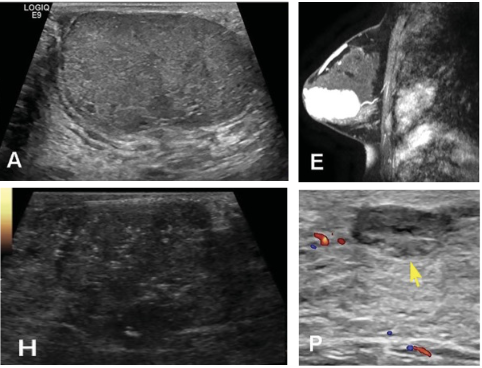
Figure 1: Imaging evaluation before and after MWA in one benign breast lesion case [7]. (A) BBL with 6.0cm * 3.5cm * 4.9cm size showing hypoechogenicity with a clear margin on US. (E) Contrast-enhanced MRI showing a hyper-enhancement in the benign breast lesion parenchyma in the arterial phase before MWA. (H) After MWA, a hypoechoic ablation zone with a size of 5.0cm * 3.6cm * 4.5cm is shown in the tumor region by CEUS. (P) After 12 months follow-up, the ablation debris decreased gradually to a size of 1.1cm * 0.4cm * 1.2cm on T2-weighted images (yellow arrows in P).
Advantages













 Video
Video